







- The American Lung Association founded the INDEPTH™ Diversion Project, which is a convenient alternative to suspension or citation that helps schools and communities address the teen vaping problem in a more supportive way. Instead of solely focusing on punitive measures, INDEPTH is an interactive program that teaches students about nicotine dependence, establishing healthy alternatives and how to kick the unhealthy addiction. INDEPTH was piloted at 11 schools across the U.S. with 60% of student participants reporting that they were willing to quit using tobacco products after completing the program.
- As a natural complement to INDEPTH, schools seeking to implement teen tobacco cessation programs can sign up for the Not On Tobacco (N-O-T) program. The N-O-T Program is a voluntary, teen-centered cessation program addressing all tobacco product use, including e-cigarettes.
- The Truth Initiative specifically targets youth vaping cessation and uses the “This is Quitting” Program.
- Aspire Program, released by MD Anderson Cancer Center, is a youth-focused, bilingual program aimed at supporting teens to live a healthy, tobacco-free life.
- The Missouri Partners in Prevention provides resources, counseling and support for college students in Missouri looking to quit using tobacco and/or marijuana through their Make a Change program. This program offers counseling and nicotine replacement therapy, as well as campus-specific resources.
- Smokefree Teen by the National Cancer Institute offers several tools and tips for youth and young adults along their quitting journeys, including text messaging, cessation coaching and Instagram connections. Smokefree Teen provides support apps, coaching and a personalized quit plan.
- NOT for Me is a six-week online program offered by the American Lung Association that allows tobacco users to access the resources and support they need. The program helps participants understand their relationship with tobacco and gives them the tools they need to quit.
- This is Quitting is a text-to-quit program from the Truth Initiative that provides e-cigarette and vape users with three to five text messages per day to provide support and encouragement along their quit journey. Text DITCHVAPE to 88709.
- Tobacco EDU, developed by PEERS Against Tobacco and the University of Texas at Austin, is an interactive, web-based, self-paced curriculum for college students that includes videos, quizzes and interactive games. This chapter-by-chapter educational tool provides a certificate upon completion and is a great tool for instructors to utilize in their classrooms. Tobacco EDU discusses cigarettes, e-cigarettes, smokeless tobacco and alternative tobacco.
- Behind the Haze is an evidence-based campaign by Rescue that aims to inform young adults about factual information related to the harms of nicotine and vaping.

12.09.21
Integrating a 100% Smoke-Free Policy
Expert

Shawn Billings
Vice President of Substance Use Programming
Actions
Type
Guides
Topic
- Health Policy
- Substance Use Disorder
Tags
guide
health policy
substance use disorder
vaping
100% Smoke-Free: Integrating Vaping Into Existing Hospital Tobacco and Smoking Policy
Missouri hospitals project a healthy image in their communities, and adopting a tobacco-free or smoke-free hospital campus is one way to demonstrate this commitment to health.
This supplement to the Missouri Hospital Association’s 2005 resource, “Creating Tobacco-Free Hospitals,” provides updated tools and resources for Missouri hospitals, which are working to address the use of tobacco, e-cigarettes and vaping products.
MHA recommends expansion of existing hospital tobacco-free or smoke-free policy to include regulating and restricting the use of vaping products.
Background
E-cigarettes are battery-powered devices used to “vape” a flavored solution. E-cigarette liquid, referred to as “e-juice,” nearly always contains nicotine, an addictive chemical derived from tobacco. The use of e-cigarettes remains largely unregulated by the U.S. Food and Drug Administration and has grown significantly in popularity since 2005, presenting public health concerns about increased incidence and the prevalence of nicotine addiction.
While e-cigarettes have been considered to help people quit smoking combustible cigarettes, evidence from the Centers for Disease Control and Prevention shows that they are highly addictive and contain substances that are harmful to fetuses, young adult brains and everyone’s lungs. Research has shown that more people transition on to combustible cigarettes through e-cigarettes than transition off combustibles by using e-cigarettes. Additionally, dual use of both cigarettes and e-cigarettes is very common. E-cigarettes now are the most common tobacco product used by youth and young adult populations.
- E-cigarette companies can legally promote these products by using techniques that cigarette companies have not been able to use since the 1998 Master Tobacco Settlement Agreement, including television and radio ads, billboards, outdoor signage, and sponsorships.
- E-cigarettes are NOT approved by the FDA as an aid to quit smoking.
- E-cigarettes largely are unregulated by the FDA, and flavors have not been regulated until recently. While the FDA is taking some action on regulating flavors, most restrictions are coming from a state and local level.
- E-cigarettes are available in many flavors (bubble gum, chocolate, peppermint, etc.) that appeal to youth. Flavors, designs and marketing renormalize and glamorize smoking.
Beginning in early 2019, the CDC began to track multistate reports of vaping-related lung illness and injury, and coined the term EVALI, which stands for e-cigarette or vaping product use-associated lung injury. As of February 2020, the CDC has found more than 2,807 cases of EVALI in all 50 states, with 68 deaths spanning 29 states. The CDC developed a tracking website and provides weekly updated information to assist public health and health care providers in preventing and treating EVALI.

Proposed Policy Adjustments
MHA recommends the expansion of hospitals’ existing tobacco-free or smoke-free policies to include regulating and restricting the use of all tobacco products, including e-cigarettes. A sample e-cigarette regulation is available.
The Effects of Nicotine
The effects of nicotine remain well-documented. It is important to note that when health care professionals were interviewed regarding their patients, nicotine ranked as the most addictive substance (above methamphetamine and heroin), as well as the most difficult to stop using.i
The use of e-cigarettes is not safe, and the products nearly always include nicotine, as well as particulate matter, heavy metals and flavorings including diacetyl.i, ii, iii We must acknowledge that e-cigarettes may prove mildly safer than long-term smoking; however, safer does not equate to safe.
The effects of second and thirdhand smoking also are well known. The effects of secondhand vapor are less studied at the present time. It is important to note that while the CDC is studying the causes of EVALI and associated death, a common theme is emerging, pointing to vitamin E acetate. CDC findings suggest that EVALI cases have stemmed from patients vaping both nicotine and tetrahydrocannabinol, the common thread is vitamin E acetate. This finding reinforces that vaping is not a safe alternative, and hospitals should regulate the use of such products at their facilities.
The Tobacco Toll
- Use of tobacco and tobacco-related products remains the leading preventable cause of death.
- Tobacco use impacts every system or organ in the body.
- Tobacco use causes the deaths of 11,000 Missourians each year.
- Nearly one in five, or 19.4%, of Missouri adults smoke (921,400). The national smoking rate is 13.7%.
- Vaping among high school students has increased 78% from 2017 to 2018.
- High school students in Missouri smoke at a rate of 10.9%. National high school smoking rates are 5.8%.
- Missouri’s tobacco tax is the lowest in the U.S.
- Tobacco use costs Missourians more than $3 billion in health care costs and costs Missouri Medicaid $644.3 million annually.
Keys to Success
The successful implementation of a policy requires that hospital leadership pioneer the direction by empowering all staff and clinicians in believing it is each person’s policy to enforce. Providing a visible presence of the policy, including signage and communication via social media, websites and throughout the hospital, is critical. Existing signage should be updated to include vapor products. The policy also should be easily searchable on the hospital website for patients or visitors.
Enforcement and Maintenance:
- Approach the 100% smoke-free policy as a health and wellness initiative.
- Collaborate with other organizations in the community.
- Form a task force dedicated to enforcement.
- Include smokers in planning the policy’s implementation.
- Anticipate the impact on other corporate policies.
- Define your boundaries carefully and include all hospital grounds.
- Allow for plenty of lead time, but don’t phase the policy in — act now.
Creating and Sustaining a Supportive Environment for Enforcement and Compliance:
- Take a compassionate approach when interacting with smokers.
- Document and track smoke-free policy and cessation prior to and after implementation.
- Be consistent.
- Include all employees, patients and visitors when enforcing the policy.
Effective Communication Sets the Tone:
- Communicate early and often.
- Inform the health care community of the policy as soon as possible.
- Word your signs carefully, and update signage as needed.
- Solicit input from neighbors and the local community.
- Inform your vendors and contractors.
Enforcement Tips and Techniques:
- Foster a nonconfrontational approach.
- Stand firm and be consistent.
Employee Support
It is not unusual for hospital leadership to become concerned about policy implementation from an employee satisfaction and retention perspective. Utilizing nicotine replacement therapy, pharmacotherapy, coaching and additional supports are the most effective strategies for assisting someone with cessation efforts. Hospitals may utilize existing resources, such as insurance coverage of pharmacotherapy and/or nicotine replacement therapy and employee assistance plans, to provide coaching. The Missouri Tobacco Quitline is another great resource to offer employees as it provides 24/7 phone and texting support. In some cases, hospitals already provide on-site cessation services and, when possible, may provide full-service cessation services during the workday to incentivize attendance and retention.
Use of progressive discipline procedures are suggested for staff who ignore or violate the policy on a repeat basis.
Patient and Visitor Support
Hospitals that are successful in integrating 100% smoke-free campuses instruct employees to approach smokers with courtesy and respect, and to foster a nonconfrontational approach to enforcement. Employees who approach visitors can politely inform them of the policy; there is no need to engage them in debate — they simply can provide information and walk away. If members of security staff are involved in enforcement, encourage them to “redirect” individuals who are seen smoking by requesting them to stop, and if necessary, directing them to locations away from the hospital.
Even organizations with the most perfectly planned and implemented policies will experience imperfect compliance or enforcement. No health promotion effort achieves 100% success, but adopting a smoke-free policy and enforcing it as consistently as possible will benefit everyone’s health and safety.
Be prepared to identify and monitor “hot spots” where enforcement may be troublesome — some areas of campus property naturally will provide more hiding places than others. Actively identify and monitor these “hot spots” where covert smoking can occur. Several areas frequently present special challenges to smoke-free policy enforcement. The area outside the emergency department is perhaps the most common. A compassionate, nonconfrontational approach can be particularly helpful here. Some hospitals choose not to enforce the policy when a distraught family member or loved one is seen using tobacco. Others take the opportunity to offer sympathy and assistance, either offering a nicotine replacement product, such as gum or lozenges, or guiding the individual to locations off the property.
In terms of patient care policies, work with inpatient units to implement standing orders for nicotine replacement so that they have an alternative to offer smokers who experience cravings while hospitalized — or who find being in a smoke-free environment is an incentive to quit.
Communication Plan

- Provide mandatory employee education with demonstrations on how to approach someone in violation of the policy.
- Ensure employees are aware of the hospital-specific resources for cessation and short-term treatment.
- When available, provide a small quantity of nicotine replacement products for visitors and patients.
- Incorporate permanent and visible signage on the grounds, entrances, parking garages and inside all facilities announcing the nicotine use policy.
- Ensure that signage is easily understood and that the message is clear, including the universal no-smoking signage.
- Flyers, calendars, social media and websites should announce the countdown to policy implementation, making clear the policy now will include vaping products.
Additional Policy Considerations
These new products and the subsequent health crisis emphasize the need for comprehensive tobacco policies. There are several other related policy considerations, including Tobacco 21 and marijuana use.
Tobacco 21 (including vaping) prohibits the sale (not possession) of tobacco before age 21. President Trump signed Tobacco 21 into law on Dec. 20, 2019, with immediate implementation. While previous legislation has been filed, Missouri is one of only 11 states that have yet to pass a statewide policy for Tobacco 21.
With the medicinal and recreational legalization movement, smoked or vaped marijuana products and secondhand marijuana smoke have been on the rise. It should be noted that there is a connection to THC and vitamin E acetate use in EVALI cases. Thus, considerations to address smoked marijuana can be explored.

Appendix
Evidence-Supported Interventions
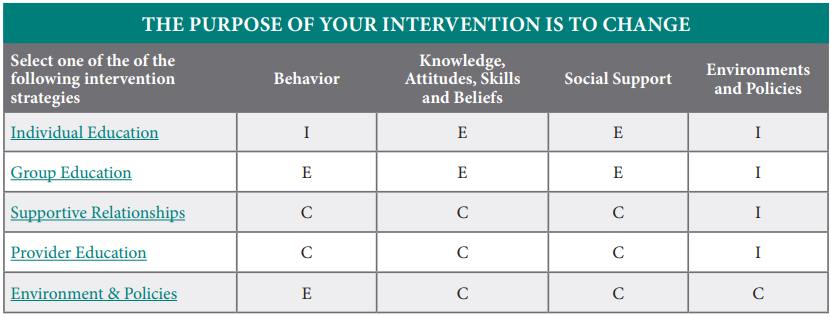
E = Evidence-based strategy
C = Evidence supports this strategy when used with other strategies.
I = There is insufficient evidence to make a recommendation.
References
i Perrine, D. M. (1996). The Chemistry of Mind-Altering Drugs: History, Pharmacology and Cultural Context. Washington, D.C.: American Chemical Society.
ii Campaign for Tobacco-Free Kids. (2020). The Toll of Tobacco in Missouri. Retrieved January 6, 2020, from https://www.tobaccofreekids.org/problem/toll-us/missouri
iii Centers for Disease Control and Prevention. (2019). Quick Facts on the Risks of E-cigarettes for Kids, Teens and Young Adults. Retrieved January 16, 2020, from https://www.cdc.gov/tobacco/basic_information/e-cigarettes/Quick-Facts-on-the-Risks-of-E-cigarettes-for-Kids-Teens-and-Young-Adults.html