Humans tend to personify. We see faces and familiar shapes in clouds, and attribute human virtues and vices to objects. It’s hard-wired into our survival systems and DNA. COVID-19 has a biology, but it doesn’t have a psychology. Nonetheless, its biology can and will have short- and long-term consequences on our psychology.
COVID-19 is known to cause fatigue. However, through the long arc of our response, there is another COVID-19 fatigue that we expect to be more pernicious. Our response has reduced many of the most human of activities and, in the worst cases, resulted in lonely deaths, isolation, a reduced sense of community and limits on our interaction with even the most intimate of family and friends.
Monday, MHA and the Missouri Department of Mental Health held a joint webinar on the behavioral health links to the COVID-19 crisis. It was eye opening. Not just about the disease, but about the disease’s influence on the behavioral health system. As evidenced by this webinar, Missourians have a proactive mental health department that is committed to the health of everyone in the state.
And their work couldn’t be coming at a more appropriate time. The American Psychological Association this week released their “Stress in America 2020: A National Mental Health Crisis” report. The report, “found that nearly eight in ten adults (78%) say the coronavirus pandemic is a significant source of stress in their lives, while three in five (60%) say the number of issues America faces is overwhelming them.” The report goes on to say that, “nearly one in five adults (19%) say their mental health is worse than it was at this time last year.”
The challenge to everyone is evident, but for health care providers it is two-fold. First, members of the hospital team have been responding to COVID-19 for months, and the significant stress related to the duration of the response, patient care and organizational dynamics, and the challenges that they feel at home as members of our communities has been overwhelming. Second, we know that Missouri was experiencing a variety of behavioral health challenges prior to COVID-19 — provider shortages, substance use disorders and significant demand for all types of behavioral health services.
As we move into late fall and winter — with reduced opportunities for time outside, socially distanced interactions and the holiday season — these behavioral health challenges are likely to compound. DMH indicates that their systems have seen an uptick in contacts to their various behavioral health intervention systems. The pressures on our workforce and communities will multiply in late 2020 and throughout 2021.
The COVID-19 crisis now is especially acute in rural parts of the state. While the virus had limited impact on rural Missouri initially, despite several outbreaks in meat packing and other agricultural processing facilities, it now has taken hold on a much larger scale. Hospitals that provide local and regional hub care for these communities are significantly stressed. And, many rural communities have yet to put strong public health protections in place to limit the spread.
In February, MHA, along with several partners, released a report, “Growing Stress On The Farm,” outlining the significant behavioral health challenges in rural communities. These challenges preexisted COVID-19, and are likely more profound today. According to our research, “Pervasive stigma and geographic barriers to accessing mental health care can prevent all who seek behavioral health services in rural Missouri from seeking help for stress, anxiety and depression. Each of Missouri’s 99 rural counties is a designated Mental Health Professional Shortage Area, and with just 3.7% of the recommended supply filled, Missouri faces the largest shortage of behavioral health care providers in the U.S.”
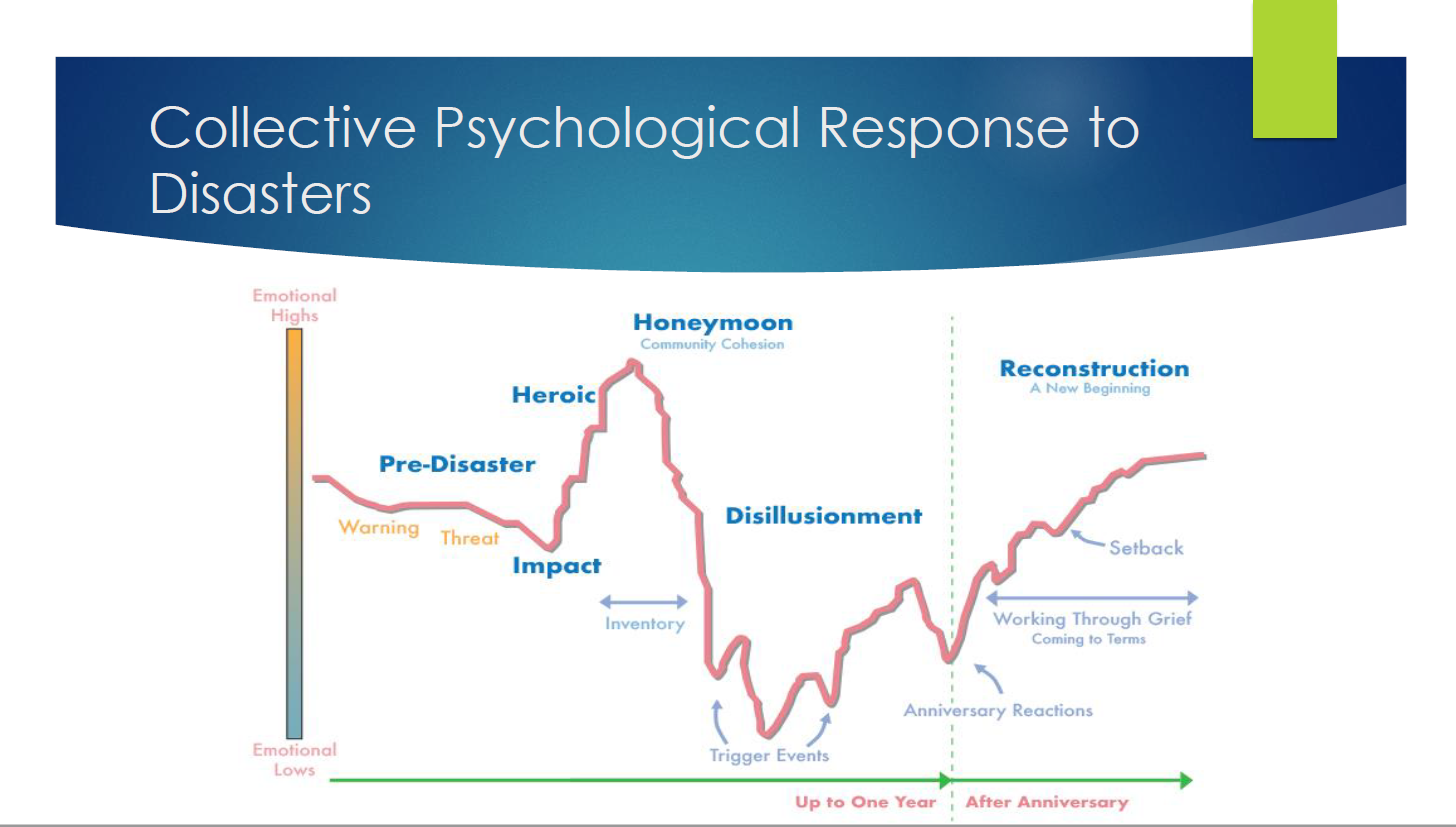
There are no easy solutions to the behavioral crisis that is lurking immediately below the surface of the COVID-19 crisis. It will not be limited to rural communities or members of the health care family. It will, however, persist. A chart from the webinar exposes the long path to behavioral health recovery from a crisis. It is chilling.
As I’ve been thinking about where we are with the crisis — especially in our health care system and among our rural communities — I’ve been reminded of the words on the Missouri State Flag. “United We Stand. Divided We Fall.”
Humans see faces everywhere, even where there are none. We make judgements using primitive parts of our brain, even when situations are complex. We can’t often tell by the simple signals whether something important is happening behind an expression — and now that expression may be behind both a literal and figurative mask.
As leaders, we endeavor to take care of our people and our communities. We know what’s coming or even what is already here. The virus is running roughshod on our physical health in communities throughout Missouri. But, it’s also influencing our mental health. Let’s not let our work healing bodies mask the next challenge.
Missouri’s Congressional Delegation Supports COVID-19 Relief Fund Repayment Changes
MHA Produces Toolkit For Expanding Hospital Capacity
FDA Approves Gilead’s Remdesivir As Coronavirus Treatment
CDC Study Indicates Higher Risk Of In-hospital Complications For COVID-19 Versus Flu
CMS Delays The Radiation Oncology Model
HealthCare.gov Premiums Lower For Third Consecutive Year
MLN Connects Provider eNews Available
DHSS Announces New Changes For CNA Testing
Brave Of Heart Fund Available To Families Of Health Care Workers
The U.S. Department of Health and Human Services announced updates to the September guidance that set reporting and repayment expectations for the Provider Relief Fund payments. HHS states, “HHS is amending the reporting instructions to increase flexibility around how providers can apply PRF money toward lost revenues attributable to coronavirus. After reimbursing health care-related expenses attributable to coronavirus that were unreimbursed by other sources, providers may use remaining PRF funds to cover any lost revenue, measured as a negative change in year-over-year actual revenue from patient care-related sources.”
HHS is revising the standards based on the concerns raised by many stakeholders, including most of Missouri’s congressional delegation, and MHA and its members. On Oct. 22, seven of the eight U.S. representatives from Missouri signed a joint letter urging HHS to replace its new standards for using and repaying PRF funds with the agency’s June directives. Two hundred sixty-six members of the House of Representatives sent the letter; 218 is a majority. They join a majority of the U.S. Senate, including Sens. Roy Blunt and Josh Hawley, who previously sent separate letters on this topic. MHA appreciates their response to hospital advocacy on this topic.
The Missouri Hospital Association published a COVID-19: Expanding Hospital Capacity Toolkit to help hospitals plan for and manage surges of COVID-19 patients. As the pandemic response continues — coupled with the resumption of elective surgeries and procedures, increased patient confidence with resuming health care activities, and changes in post-acute testing and tracing activities — the capacity within the hospital may become limited for periods of time. This document focuses on capacity building and patient throughput processes to continue care for an increased volume of patients. While this document focuses on increasing physical capacity, MHA also offers considerations for maximizing workforce in the COVID-19 Surge Staffing Solutions Fact Sheet.
In May, the U.S. Food and Drug Administration granted remdesivir as an emergency use authorization, allowing hospitals and doctors to use it on patients hospitalized with the disease even though the medication had not been formally approved by the agency. The intravenous drug has helped shorten the recovery time of some hospitalized COVID-19 patients. The drug will be used for COVID-19 patients at least 12 years old and requiring hospitalization, Gilead said. Remdesivir now is the first and only fully approved treatment in the U.S. for COVID-19.
The Centers for Disease Control and Prevention issued a new study this week indicating that hospitalized patients with COVID-19 had more than five times higher risk for in-hospital death and increased risk for 17 respiratory and non-respiratory complications than did hospitalized patients with influenza. The risks for sepsis and respiratory, neurologic and renal complications of COVID-19 were higher among non-Hispanic Black or African American and Hispanic patients than among non-Hispanic White patients.
The Centers for Medicare & Medicaid Services is delaying the Radiation Oncology Model implementation date from Jan. 1 to July 1, 2021. The delayed implementation date is due to feedback from stakeholders who expressed the challenges of preparing to implement the RO model during the public health emergency.
The Centers for Medicare & Medicaid Services released a report that shows a continued trend of lower premiums and increased issuer participation for HealthCare.gov in 2021. According to a CMS report, the average second lowest cost silver plan is expected to decrease by 2% in Missouri. CMS Administrator Seema Verma stated, “Bottom line – The President has delivered, lower cost and more choice. Our changes to the regulations and how we have managed the exchanges have proven to be more effective than previous administrations.” CMS also provided the following information.
The Centers for Medicare & Medicaid Services issued updates to MLN Connects Provider eNews. eNews includes information about national provider calls, meetings, events, announcements and other MLN educational product updates. The latest issue provides updates and summaries of the following.
opioid use disorder treatment: Medicare coverage
clinical diagnostic laboratory tests advisory panel: request for nominations
Medicare Part A cost report: new bulk e-Filing feature webcast – Oct. 29
The Missouri Department of Health and Senior Services Health Education Unit announced new changes for CNA testing beginning in December. Headmaster D & S will be the test administrator who will manage testing for all students taking the knowledge and skills tests. DHSS has scheduled several Q & A sessions, hosted by DHSS & Headmaster D & S, and ask that you view the Missouri Nurse Aide Competency and Evaluation Webinar prior to attending. Please call 573-526-5686 or email cnaregistry@health.mo.gov with questions regarding the new transition.
The Brave of Heart Fund was created by the Foundations of New York Life and Cigna with charitable partner, E4E Relief. The Brave of Heart Fund provides financial grants to families of eligible health care workers, volunteers and support staff who lost their lives in the fight against COVID-19. For a list of eligible workers, please see the FAQ.
To date, the Fund’s activity includes more than $5.4 million in charitable grants that have been awarded to more than 180 families. The grants provide basic and continuing financial support for common needs such as funeral costs, medical care, counseling, food, education, mortgage/rent payments and immediate living expenses. The grantees have primarily been the spouses and dependent children of deceased health care workers and volunteers.