








06.06.18
Newborn Opioid Withdrawal Potentially Undercounted
Expert

Dave Dillon
Actions
Type
Topic
- Maternal Health
- Opioids
- Substance Use Disorder
Tags
The number of newborns suffering withdrawal from maternal opioid use during pregnancy could be significantly larger than previously estimated, leading to significant direct and indirect costs to care for these children, in both the short and long term. New research from the Hospital Industry Data Institute, the data company of the Missouri Hospital Association, examines the prevalence of neonatal abstinence syndrome in the state, estimates costs for medical care and social services, and offers policy solutions to reduce the incidence and costs through maternal care management.
More than half of all babies born to mothers who either misused or were prescribed opioids to manage pain during pregnancy suffer from NAS. Opioid use can harm a developing fetus and lead to withdrawal symptoms after delivery. In addition to the human cost, there is a high health care cost. The average length of stay for a NAS newborn is 10 days longer than a non-NAS newborn. Moreover, the average hospital charge for a delivery in Missouri is $5,000, but NAS-related care averages $33,000 per child — a 570 percent difference.

Missouri’s Medicaid program pays for 83 percent of NAS deliveries, nearly twice the rate of non-NAS deliveries. Using existing prevalence data, Medicaid’s estimated additional hospital costs associated with NAS births was $10 million in 2016. These costs don’t include the additional downstream health care, social services and educational investments. However, evidence suggests that the incidence of NAS is underreported, and the cost could be much larger.
“Understanding the scope of the NAS problem is the first step in identifying solutions,” said Herb B. Kuhn, MHA President and CEO. “The existing data didn’t correlate well with what clinicians were reporting from the front lines of care. To identify inconsistency, our researchers identified potentially correlated data and surveyed Missouri’s birthing hospitals to evaluate NAS prevalence through a different prism.”
Rep. Holly Rehder of Sikeston has been a leading voice in the Missouri General Assembly on the opioid crisis. She has advocated for state legislation to mitigate the harm to individuals and communities.
“No baby should be born withdrawing from an opioid,” Rehder said. “I’ve seen the high cost of drug abuse in my family and in the community I serve — it’s personal. This new research shows that our fight to curb the opioid crisis, and to protect newborns, will require work by all stakeholders. There isn’t a single solution. The crisis demands that we look at all options.”
Researchers conducted two analyses drawing from alternative data sources. First, new and expecting mothers’ hospital discharge data for opioid-related hospital inpatient and emergency department care were reviewed for nine months before and after birth. Second, a survey of hospital obstetric health providers gleaned observational data, including perceived prevalence and severity of NAS in Missouri OB departments.
During 2016 and 2017, conventional surveillance identified 1,083 Missouri newborns diagnosed with NAS. However, discharge records for new and expecting mothers found 3,714 women with at least one hospital visit for opioid misuse during the two-year period. For women who gave birth during the study period, 56 percent had an opioid-related encounter during gestation, with 62 percent occurring in the third trimester and 25.6 percent on the day of birth.
More than half of Missouri’s birthing hospitals participated in the survey. These hospitals account for 45 percent of all Missouri births and 50 percent of all NAS diagnoses. The reported perception of NAS severity at surveyed hospitals correlated with conventional data. However, significant disagreement was found between hospital-diagnosed and coded NAS and survey-reported prevalence — a range of 2.8 to 20 times higher than the rate identified through conventional diagnosis codes.
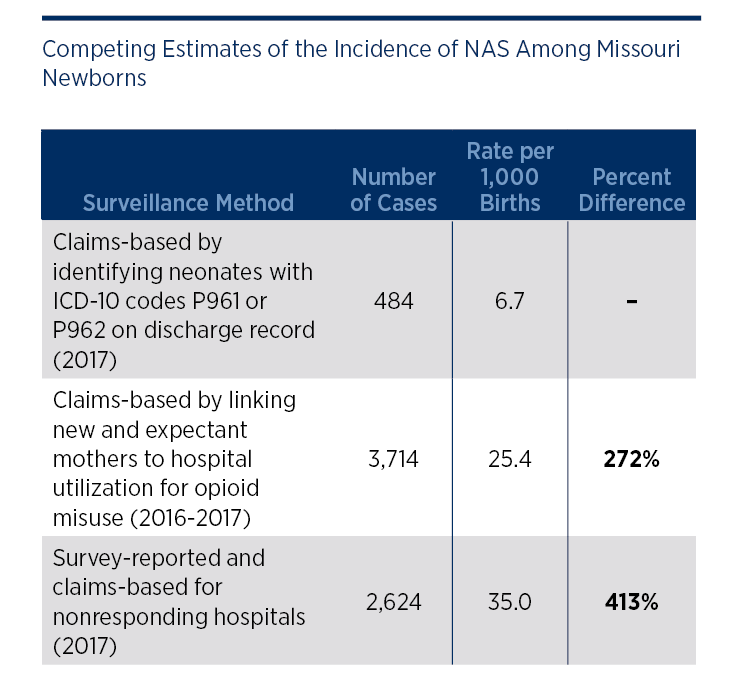
When comparing the three competing estimates of NAS prevalence, a wide range of variation was identified. Claims-based analysis of maternal opioid use during or after pregnancy yields an estimated 3,714 cases, while survey-reported cases are estimated at 2,624. Traditional surveillance yields only 484 cases during 2017.
“Using conventional measures, NAS is outpacing the other consequences of the opioid crisis, including mortality and increased hospital service utilization,” said Kuhn. “This research indicates that the problem is likely much larger than previously understood. The only way to reduce the incidence of NAS is to reduce opioid use during pregnancy. That will require better coordination and increased investment in access to treatment for substance use disorder and supportive social services.”
The policy brief identifies how providing evidence-based opioid use disorder treatment to low-income, uninsured women of childbearing age with substance use disorder prior to pregnancy could reduce the medical and societal costs associated with NAS. Through a federal waiver, substance abuse treatment could be made available through Medicaid that is revenue neutral. The proposal would use cost avoidance for NAS-related care to redirect spending for substance abuse treatment. This would reduce state and federal spending in other areas as well, including foster care, and create a cumulative savings of approximately $14.5 million throughout a decade.
“Reducing NAS by eliminating the upstream cause of maternal opioid abuse makes sense for mothers and babies, and is fiscally responsible,” Kuhn said. “Prevention could reduce harm to the most vulnerable victims of the opioid crisis.”